For World Suicide Prevention Day, I tweeted that people could ask me anything about suicide. Thanks to everyone who already sent me questions – they’re really good ones! If you want to submit a question, tweet it to me (@DrKathrynGordon) or e-mail it to me (kathrynhgordon@gmail.com).
If you’re in crisis, please contact the National Suicide Prevention Lifeline or the Crisis Text Line. The responses below are my opinions and should not to be taken as professional advice. More suicide prevention information and resources are available here.
Added September 11, 2019
Anonymous asked: What criteria do mental health professionals use when deciding whether someone should be admitted to a hospital involuntarily for suicide risk?
Laws vary by location, and the criteria depend on the particular mental health professional, client, and situation. The typical criteria for involuntary hospitalization is that the person is at imminent or immediate risk for suicide. The field has a lot of work to do to get better at predicting when someone is at immediate risk for suicide (e.g., see Franklin, Ribeiro, et al., 2016). Some factors that therapists tend to view as indicative of immediate risk for suicide include (e.g., see Chu et al., 2015):
- a clear, resolved plan and/or preparations made for suicide, intent to act on the plan, and access to lethal means (or plans to acquire lethal means)
- multiple past suicide attempts (especially if recent)
- the therapist and patient cannot create an alternative plan for safety (e.g., staying with a friend, temporarily storing lethal means elsewhere, identifying ways of coping with emotional pain that don’t involve suicide)
The mental health professionals who I have interacted with over the years tend to be eager to find alternatives to involuntary hospitalization. They seek to respectfully and collaboratively create a safety plan with their clients. However, I know from listening to other people’s stories that it’s not always the case. For example, Rudy Caseres is a mental health advocate who has spoken and written about these issues, and I recommend checking out his website here.
Published September 10, 2019
@ToWit12 asked: Let’s go worst-case scenario, where I encounter someone already with a gun to their head or about to jump off a bridge. What is the right (or rather, least wrong) thing to say/do?
Most people in that kind of emergency situation are experiencing pain, loneliness, and hopelessness. Individual situations vary quite a bit, but this would be my default:
I’d ask them to put the gun away or step away from the bridge, so we can talk (to increase safety). I’d talk to them in as calm and warm of a tone as possible. I wouldn’t endanger myself in this process, say they’re bluffing, or ignore them. I’d call for help if I could (911). I’d tell them I care about them, and that I’m there to listen and not to judge them. If I had struggled in my life, I’d let them know that (to increase a sense of connection). I’d commit to helping them find resources for addressing their problems (to increase hope).
For more on this topic, I recommend listening to this Story Corps segment about a police officer (Kevin Briggs) who helped a man (Kevin Berthia) who was about to jump off of the Golden Gate Bridge. It’s also worth watching Kevin Berthia’s TEDx Talk, The Impact of Listening and listening to this NPR segment, Mental Health Cops Help Reweave Social Safety Net in San Antonio for their approaches in mental health crises.
—————————————————————————————————————————
Anonymous asked: I developed PTSD in the course of supporting a suicidal friend. Now other people’s suicidality is triggering to me, and I expect it to be that way for a while. I want to support friends who need it, but I want to support them at arm’s length. I’m in no position to be in the front lines of anyone’s mental health support team. This has been a problem: having gone to bat for one suicidal friend, I seem to be socially marked now as a person who will be supportive, even among people who are intellectually aware that it traumatized me. I’ve been somewhat beset by men, in particular, who demand that I provide womanly sympathetic listening without regard for my own mental health. Dealing with this gently while managing my PTSD symptoms is challenging.
World Suicide Prevention Day is coming up and I dread it. This is the kind of season in which I’m approached directly for mental health support that I’m not in a position to give.
I want to set very firm boundaries about how much mental health support I’m willing to do, preferably without hurting or antagonizing extremely sensitive people or getting into any arguments about whether I’m an ableist who’s contributing to stigma. How do I do that?
First of all, I’m very sorry that you had to go through such a painful experience. I hope that you have been able to find effective treatment for your PTSD.
Secondly, in my work as a therapist, I’ve heard a useful analogy used about helping others. When you’re on an airplane next to a child, they tell you that you need to put on your own oxygen mask in an emergency situation before assisting the child. If you don’t, you could suffocate while trying to put the mask on the child, and then neither of you will survive.
Right now, it sounds like putting on your own oxygen mask first means not being available to others in suicidal crises. I would say something like this, “I see that you’re in a lot of pain, and I really feel for you. I can’t be the one to support you right now. I’m struggling too, and to be well, I really need to focus on working through that first. If you can’t think of anyone else to talk to, you can always contact the National Suicide Prevention Lifeline. I hope you find the support that you need.”
My hope is that most people would respond to that in a positive, understanding way. However, if they perceive your response as ableist, stigmatizing, or anything else like that — it’s important to stick with your boundaries anyway (repeating what you said, if necessary). We can’t control what other people think of us, but we can do our best to live according to our values and strive to be okay with our own decisions. Your mental health matters, and good friends should support your decisions to take care of it.
—————————————————————————————————————————
Zach Clement asked: How can I support a friend who is considering suicide while keeping myself emotionally healthy, and how do I disengage with them when my relationship with them becomes unhealthy for me?
I recently was trying to give support to someone because I knew they were having a hard time, and they had said that they thought about killing themself. However, as time went on, they started attacking me and my relationships with others. I realized that my only reason for talking to them was that I knew I would feel guilty if I didn’t. Eventually, I told them that I wouldn’t talk to them anymore if they continued to attack the things that I valued, and they didn’t stop, so I told them I would just ignore them. I offered to help them find a therapist when I cut things off with them, but I still sometimes feel like I should have done something differently.
This is a really tough situation, and I don’t think these potentially complicating factors are included enough in public discussions of suicide. It sounds like you told the person how they were affecting you and gave them chances to apologize and change their behavior. Unfortunately, the person didn’t. A natural consequence of someone attacking you and your relationships with others is that you’re going to want to distance yourself from that person. And no amount of the other person’s pain gives them a right to be abusive toward you.
Honestly, I think I would have done the same thing that you did. I’d tell them that I couldn’t keep being around them if they treated me like that, but that I wanted to help them get connected with a therapist. The fact that you offered that was very kind and above and beyond what most people would do. I might give them some additional information like the National Suicide Prevention Lifeline. If I knew someone else close to them – and it fit with the situation – I would mention that the person brought up suicide before and that you’re concerned.
I’d probably feel a bit unsettled about the situation, because I’d worry if the person hurt themselves I’d feel responsible. From my perspective though, you can’t allow someone to treat you like that repeatedly because you feel guilty. It sends the message to the person that it’s okay for you to be treated that way or that it’s okay for you to suffer because they are. So, then I’d try to cultivate some acceptance about the limits of what I can do for the person. It sounds like you made a healthy and correct decision for yourself. I hope the person pursues professional help and that you feel at peace with the way you handled it.
—————————————————————————————————————————
Tyler Pritchard asked: Who are your top 3 influences in suicidology research and/or practice?
- Without a doubt, the most influential person in my scientific and clinical work is Thomas Joiner. He was my research mentor during undergraduate and graduate school. Thomas also directed my graduate program’s training clinic and played a huge role in my development as a therapist. His compassion, intellectual curiosity, and direct approach are all qualities I admire and strive to bring into my work.
- Marsha Linehan created a therapy for people who were traditionally excluded from clinical trials (e.g., high suicide risk, multiple mental health issues) with an empathic, skills-based approach. Her courage, irreverence, and dedication to helping people build lives worth living inspires me.
- It’s hard to pick the third person, so I’ll say my former grad school labmates as a group (e.g., Kim Van Orden, Tracy Witte, Jill Holm-Denoma, April Smith, Ted Bender, and Mike Anestis). They’re brilliant scientists and clinicians and also exceptionally kind people. Conversations with them over the years have helped me to understand suicidology at a much deeper level than I would without their friendship and collaboration.
Even though I already exceeded the 3 with that last one, I’ll also mention David Klonsky. The way he thinks about science and his 3-step theory of suicide have influenced me a lot too.
There are a bunch of others that come to mind, but you didn’t ask for my top 300, so I’ll stop here. 🙂
—————————————————————————————————————————
Mike Heady asked: I’m not sure you have an answer for this but here it goes. I’m looking for data on how many people present or are admitted to hospitals for suicide risk when in fact the person is having intrusive self-harm OCD.
Unfortunately, I didn’t have any luck finding data on this either. This is a great question though, and I want to discuss the meaning of it for any interested readers out there.
Obsessive-compulsive disorder (OCD) often includes unwanted, distressing images or thoughts (referred to as intrusive thoughts). Sometimes, these thoughts are about contamination with germs, hurting others, or hurting oneself. You can see what this looks like in this video of an adolescent being treated for self-harm OCD symptoms.
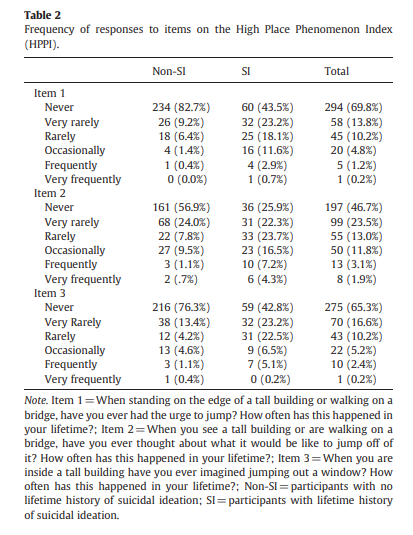
Many people — even those without OCD — have experienced a self-harm image or thought come into their mind, even when they are not suicidal. For example, Hames et al. (2012) asked a college student sample (n = 431) if they ever had an urge to jump when in a high place. They found that it was fairly common, including among participants with no history of suicidal ideation (see the table below).
For some individuals with OCD, their thoughts about self-harm are alarming, distressing, and feel like no part of what they would actually want to act on. They are not typically at high risk for suicide, because they usually try to decrease their anxiety about intrusive thoughts by taking extra safety measures (e.g., not handling knives). They’ll say that the thoughts are disturbing because they really do not want to die.
For other individuals with OCD, they may be struggling with their symptoms and considering suicide, because they believe it would be an escape from their pain. This type of situation is more worrisome.
Clinically, I’d look at the context of their suicidal thoughts to make my best judgment about their risk and whether hospital admission is appropriate. The presence of any of the following would put them at higher risk for suicide: a lack of distress or even a sense of comfort when thinking about self-harm, a history of self-harm or other suicidal behavior, a suicide plan and lack of fear about carrying it out, access to lethal means (e.g., an unsafely stored firearm), sleep disturbance, agitation, social withdrawal, severe mood disturbance, or significant weight loss.
For more information, check out this blog post: When People with OCD Fear Harming Themselves.
—————————————————————————————————————————
Anonymous asked: Suicide is a concept I am ambiguous about. When I am distressed over something after a day, or when I feel I don’t belong in society or I will never be able to function normally like other people would, I feel or think that suicide is an escape route. Like, if all else fails and pain is too unbearable to take, I could choose it. That way, I would get rid of all the things that are troubling me.
Or sometimes, I think that I am not courageous enough to pull the last act for suicide. When I brought this up during one of our sessions with my therapist, she told me that suicide is not about being courageous it is about cowardice.
So, my question is,
1 Is suicide about courage or cowardice? Does it take courage to commit suicide or does it means cowardice? Well, of course if doesn’t have to be one of those, but saying it’s cowardice feels like it’s underestimating the pain underneath. What do you think how should we look at this?
2 What do you think about the existence of the idea of suicide lingering in your head as an escape route as a comforting idea? Is it healthy, if not what can I put in its place?
1. Suicide is not an act of cowardice. Though there are different pathways to suicide, most people get there because they see no other way to escape excruciating emotional pain. They often mistakenly believe that they are doing others a favor by not living any more. Even very brave people are vulnerable to, and die by, suicide when afflicted by this pain. It’s not a sign of weakness (more about this on an NPR segment, Deconstructing Myths about Suicide).
In terms of courage – that’s not the word that I tend to use, because of it’s kind of value-laden. I prefer to describe to the ability to die by suicide as others have: capacity, capability, or fearlessness (about the pain and injury involved in suicide). For someone to kill themselves, they have to override a very strong human survival instinct. That drive to live is protective and life-saving for many people. Tragically, people who die by suicide break through that.
So, I don’t think suicide is an act of cowardice or courage in the vast majority of cases. It is an outcome that occurs when people are intensely hurting and don’t see another way out. Suicides hurt those who are left behind, even if that is not what the person intended to do. In the eyes of the bereaved, I would be surprised if they see either cowardice or courage in the situation — just heartbreak.
2. I have spoken with people personally and professionally who think about suicide to decrease painful emotions. If you’re interested, there’s some research on it in this paper called Daydreaming about Death: Violent Daydreaming as a Form of Emotion Dysregulation in Suicidality.
First, I want to say that there’s nothing to be ashamed of and that you’re not alone in doing that. It’s valid to want to decrease your emotional pain. However, I do suggest that people find other strategies for feeling better. My concern is that fantasizing about death might increase suicide risk. It could potentially reduce the protective fear that surrounds suicide and strengthen the links between positive feelings and death.
In terms of what to put in its place, you could try to imagine feeling better and that your problem is solved. If that doesn’t feel authentic or practical for you, I recommend finding ways to remind yourself of your ability to cope from past situations, that you can take things one day at a time, and that you find other ways of dealing with distress. For example, there are some ways listed in this post here that include distraction and finding emotional uplifts (e.g., watching comedy, intense exercise, seeking social support, etc.). If it’s relaxation that you are looking for, this website has some nice audio recording options that are worth trying instead. I hope you find some of these other approaches helpful and comforting.
—————————————————————————————————————————
Coral More asked: Do you see another model than assess & refer to 911/hospital given what we know about trauma resulting from police encounters and hospitalizations/emergency rooms? I know it’s a very tricky one but I never see folks talking about it.
I’ve been on both sides of this, feeling the need to call emergency services but also voluntarily presenting to the emergency room and being absolutely traumatized by the dehumanization and cruelty there.
I personally have recommended calling 911/the hospital in certain (though very few) situations where other options were exhausted and there’s urgency. These include situations where: 1) the person already hurt themselves or 2) they’re at immediate risk of self-harm. This pathway can be lifesaving, appropriate, and beneficial (though experiences vary a lot, as you said above — people can also have horrible, terrifying experiences that are detrimental to their well-being).
There are many, many more situations where I have collaboratively worked with someone to find an alternative suicide prevention approach. My default is to collaboratively create a safety and coping plan. This includes reducing access to lethal means, identifying supportive people (I often try to call at least one friend or relative with the consent of the patient, and this tends to go well), and listing methods for reducing emotional pain (e.g., emotion regulation skills, crisis survival strategies for distress tolerance). In addition, I provide them with emergency numbers, and we identify when they would need to go to the hospital or call 911 (e.g., if their suicidal thoughts escalate to suicide planning or preparation).
Part of the discussion also includes ways to intensify treatment without using the hospitalization or emergency services route. For example, increasing the frequency of therapy sessions or attending a partial hospitalization program (where people go in for treatment during the day, but sleep at home).
This article is good for looking at suicide risk as a continuum with a variety of interventions that correspond with severity: Routinized Assessment of Suicide Risk in Clinical Practice: An Empirically Informed Update.
I like what Marsha Linehan says in this video about hospitalization (keeping a person alive through constant monitoring) versus taking a risk by not always hospitalizing at any threat of suicide, so they can have a chance at building a life worth living.
I also recommend listening to Rudy Caseres, a mental health advocate, speak about his views and experiences with hospitalization in this interview.